In their preliminary analysis of the clinical parameters of COVID-19, from the first 425 patients, Li et al noted that there were no pediatric cases, and that the median age was 59 years old. While there are sure to be pediatric cases now that the total number of confirmed cases has topped 70,000, the impression has been that the pediatric age group has been very much spared a major impact from SARS-CoV-2.
Li et al surmised that perhaps the pediatric age group had some inherent resistance to SARS-CoV-2 infection via the non-specific immune response. While there is precedent for such clinical resistance in other viral infections, such as Hepatitis A and Epstein Barr virus, another explanation may lie in the annual exposure of this age group to other coronaviruses causing upper respiratory disease.
In 2018, Zhang et al published a five-year survey of upper respiratory disease in Guangzhou, to the south of Hubei province in Guangdong province, focusing on the principal upper respiratory coronavirus, OC43. Not only was OC43 circulating in four of the five years, but also throughout the year. Other coronaviruses HXU1, 229E and NL63 were less prominent, but there was an outbreak of upper respiratory coronavirus infection every year, likely continuing to this day. Furthermore, the age distribution of those viruses was markedly skewed to the very young pediatric age group.
Thus, infants in China are exposed to OC43 and other upper respiratory coronaviruses every year of their early life. It is likely that their surface immunity to these viral agents is regularly boosted.
The age distribution of OC43 is contrasted to that of SARS-Cov-2 from Li et al, adjusting the age stratification to reconcile the two studies, is shown here.
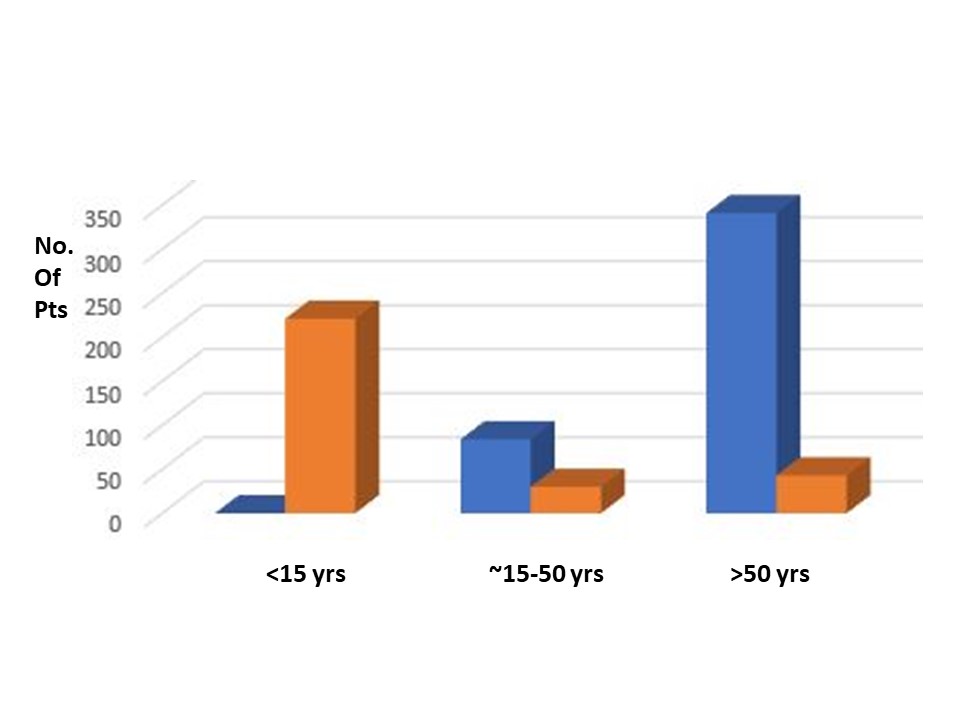
The contrast between the two age distributions could not be more stark, almost to the point of being mutually exclusive. It should be noted that both samples included hundreds of patient samples.
OC43 and SARS-CoV-2, while their sequences can be readily aligned, have little similarity in the spike S1 protein. However, they have several areas of high sequence similarity in S2, the fusion glycoprotein moiety (not shown here). One hypothesis for the marked age distribution of SARS-CoV-2 could be that the younger infant and pediatric age group is resistant to SARS-CoV-2 due to annual exposure to other coronaviruses sharing much S2 sequence, imparting secretory immunity that is not as readily reinforced in the much older age groups.
If true, such a finding would have powerful consequences for understanding the SARS-CoV-2 outbreak and how to suppress it. One corollary may be that primary and secondary schools, so often drivers of outbreaks of respiratory viruses, are not a significant factor here. I would note that two months into the outbreak, in a city of 11 million and province of 57 million, there are “only” 70,000 confirmed cases, a number concomitant with adult to adult transmission.
A second corollary could be that immunity to the more highly conserved S2, using OC43 or HKU1 as sources of immunogen, may afford a jump start on immunization of those who have not yet experienced the presence of SARS-CoV-2 in their communities.
Bill Gallaher
Refs:
Zhang S-f, Tuo J-l, Huang X-b, Zhu X, Zhang D-m, Zhou K, et al. (2018) Epidemiology characteristics of human coronaviruses in patients with respiratory infection symptoms and phylogenetic analysis of HCoV-OC43 during 2010-2015 in Guangzhou. PLoS ONE 13(1): e0191789.
Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y, et al. 2020. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. N Engl J Med. Jan 29. doi: 10.1056/NEJMoa2001316.